


How Did Cosmetic Gynecology Start
And why did it grow so fast

Vaginal rejuvenation, laser vaginal rejuvenation, aesthetic gynecology,cosmetic gynecology, cosmetogynecology, feminine restorative surgery, feminine cosmetic gynecologic surgery, plastic gynecology. Ah, so many names. It looks like the winning name of the past few years is turning out to be Cosmetic Gynecology and Cosmetogynecology. Lots of debates on this over the past couple of decades and consensus has been built. What is it? I like the way Jennifer Hays, M.D., of Clearwater, FL, states it clearly on her website:
Cosmetic Gynecology is a new sub-specialty that blends plastic surgery and gynecology. Cosmetic Gynecology or Intimate Aesthetic Surgery is a group of procedures that are cosmetic in nature and not medically necessary. They are performed to enhance the look and function of the outer vulva and inner vagina.
Marco Pelosi III, a renown leader and founder of the specialty, gave this presentation at the Baystate Medical Center, Springfield, MA, on March 20, 2013. It is an awesome dissection of the topic. Go read it.
Marco Pelosi III Presentation 3/23/13
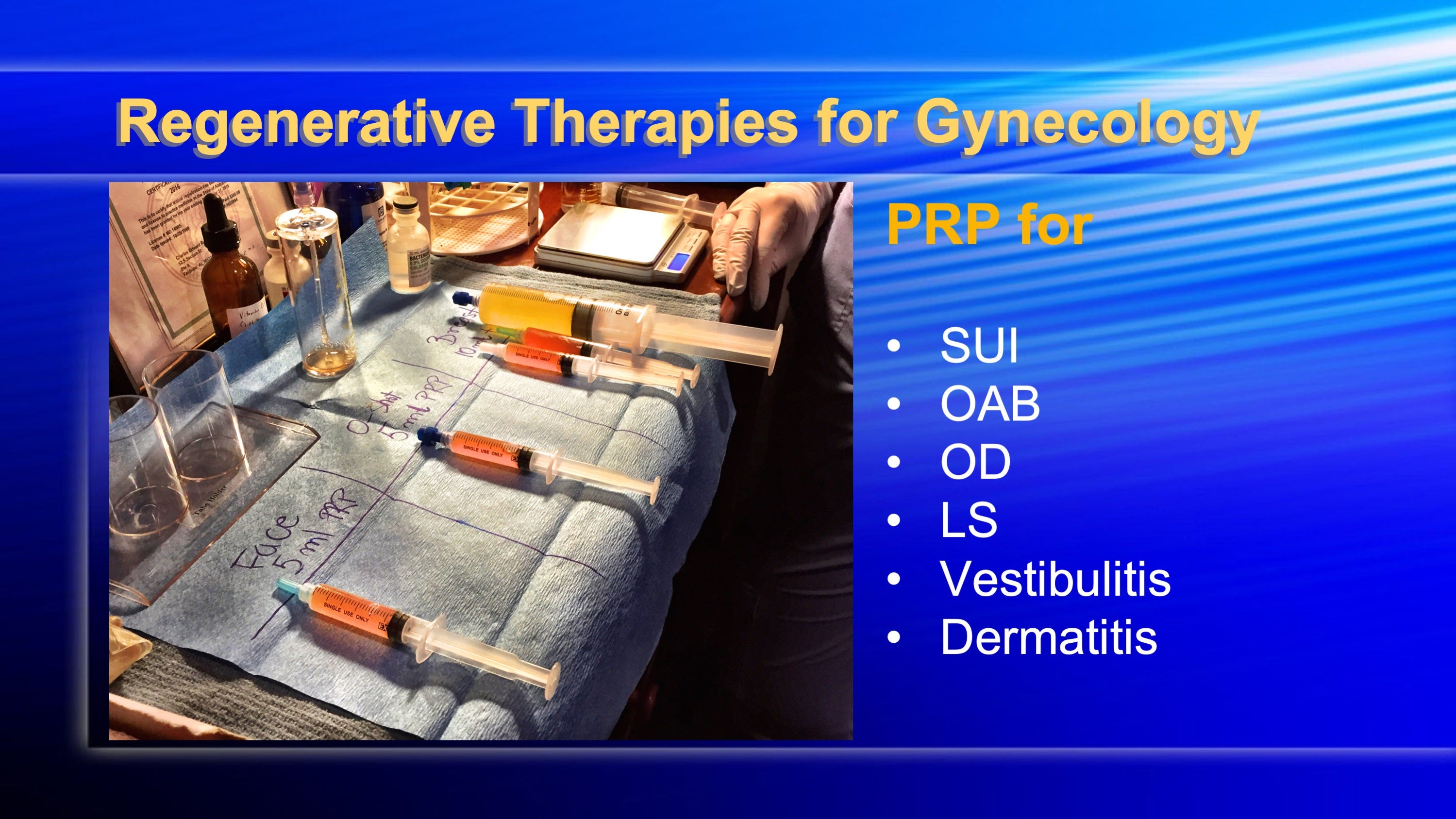
Nowadays Cosmetic Gynecology encompasses a wider field of view. Think of a plastic surgeon or cosmetic surgeon that now has gynecologic surgical skills and you approach the definition closer. Cosmetic Gynecologist do labial surgery, vaginal tightening surgeries, and more are doing tummies, breasts, and butts. All elective stuff and not necessary in medical terms. None of this is life saving surgery. And it is growing and growing and growing. Really fast. From specialties outside of gynecology! The growth of procedures from non OBGYNs such as Charles Runels O-Shot has been astounding. He has spearheaded the use of PRP for multiple gyn conditions. It was NOT a gynecologist who thought of this.
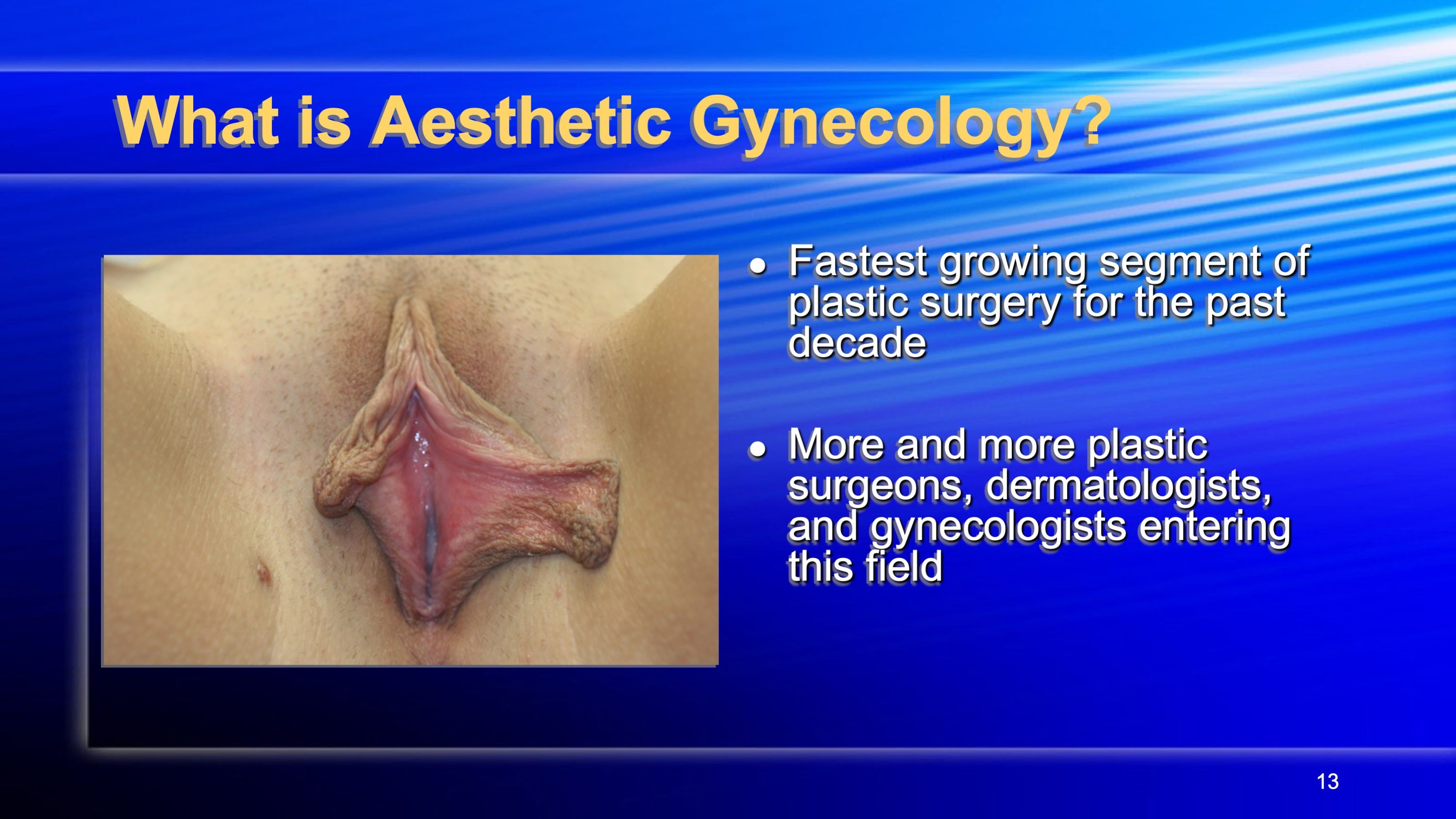
The fastest growing segment of plastic surgery this past decade. So many more plastic surgeons are doing labial surgeries than gynecologists. They embrace it, want the market. Gynecologists traditionally run away from it.
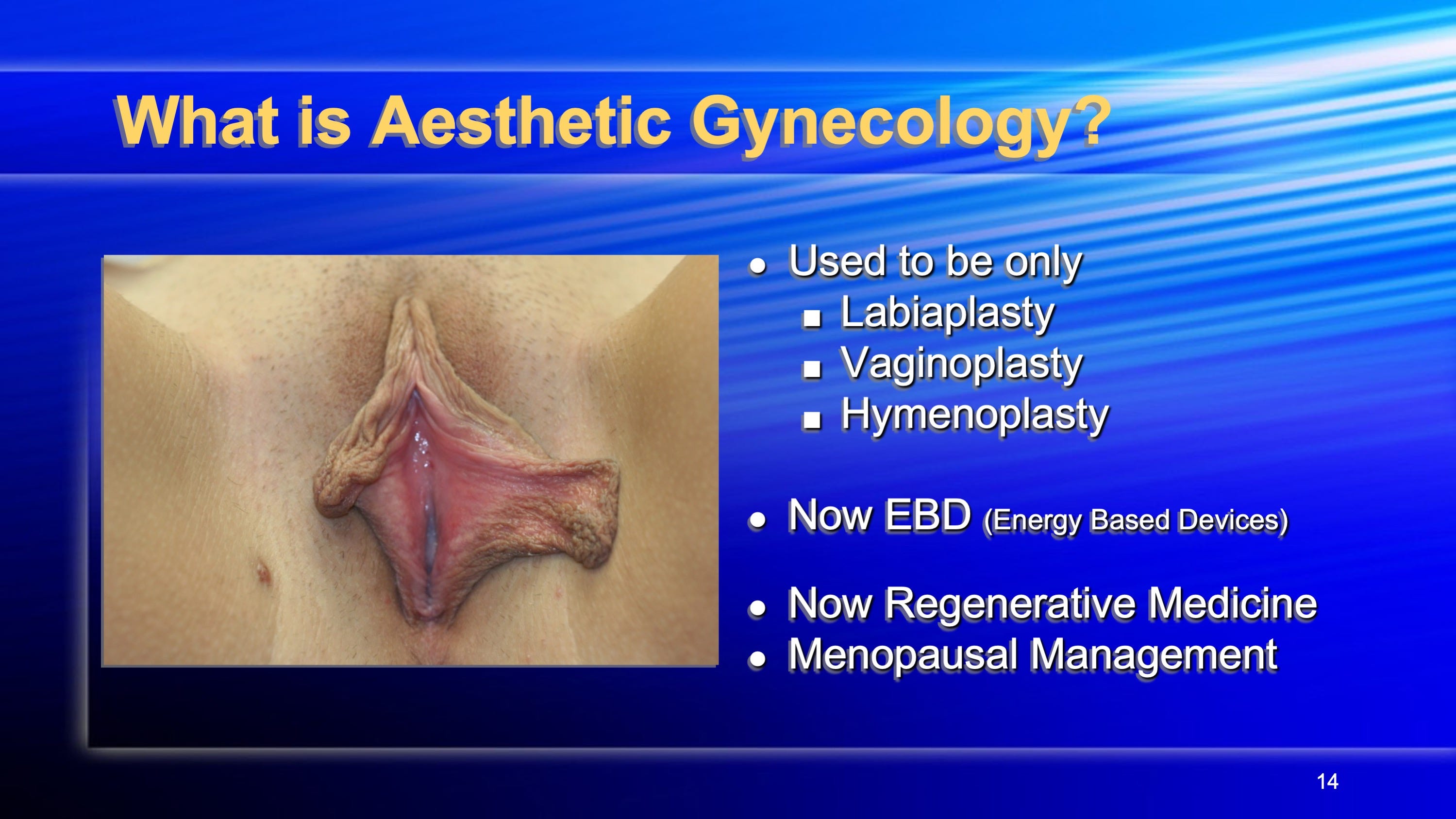
So now Cosmetic Gynecology is separated into surgical and non-surgical treatments. Not just labial surgery anymore. Not just vaginal tightening or Hymen repair. EBDs (Energy Based Devices) and Biologic/Regenerative have transformed the specialty dramatically since 2015, the year it all exploded, when ThermiVa and Viveve RF and Mona Lisa Laser entered the markets in America. So now, instead of just making the vulva and labia pretty, you could take care of problems such as vaginal dryness, loss of sensitivity, overactive bladder, stress incontinence, lichen sclerosis. The cosmesis started becoming secondary to function! Who wudda thunk that would happen! But it did! This ruffled alot of academics because the treatments were new and relatively untried and the safety was questioned. Almost a decade later and looking back, the safety and efficacy of the “questionable” treatments have been found to be gratifying. It saved many marriages, saved many despondent women, rescued many medical practices by providing options outside of the medical insurance world whose sole function was NOT to pay the doctor it seemed.
But it was hard in those early days to get the traditional OBGYN to make the jump to learn the new treatments now learned in residency and ACOG meetings. Lots of fear all around.
Our own specialty College (American College of Obstetrics and Gynecology) seemed to block all discussion on Cosmetic Gynecology for over a decade. Too taboo. They created Special Interest Group with non-experts, residents and fellows who knew little. They chose similarly minded folks to be members of the group. They stacked the deck on the debates at their Annual Meetings pitting non-experts to go at each other. Pros and Cons debates were more like Cons and Cons debate. No one who was actually a practitioner of Cosmetic Gynecology were ever invited to go toe to toe with Con debater. What were they afraid of? Loosing control.
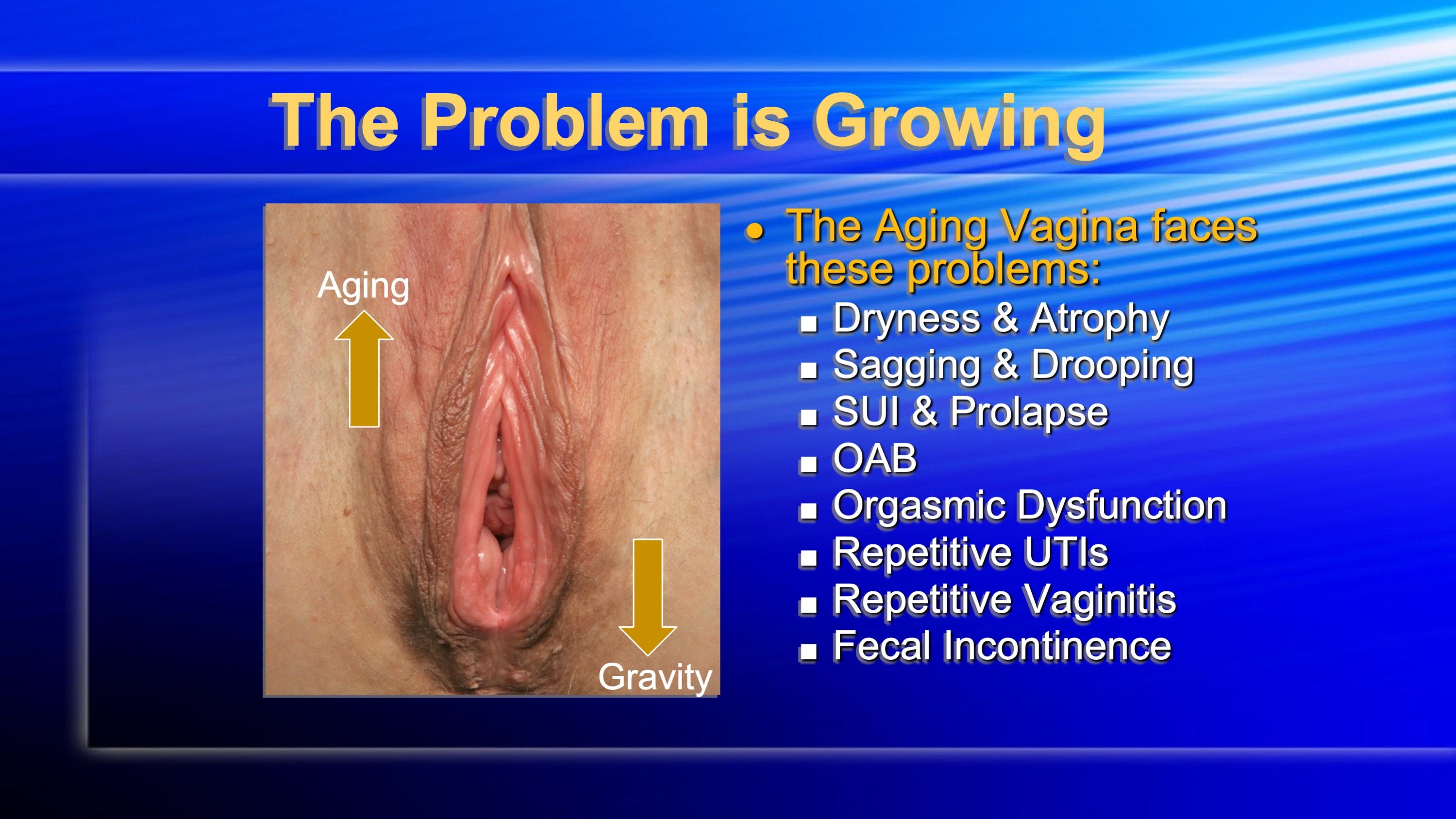
Soon doctors were figuring out that the gynecologic conditions of aging could be successfully treated with the newer therapies and that there was great patient satisfaction in doing so. Patients were willing to pay cash and not rely on insurance approved procedures only. The traditional treatments worked but now there was a growing list of options to consider! These options were changing lives for the conditions listed below.
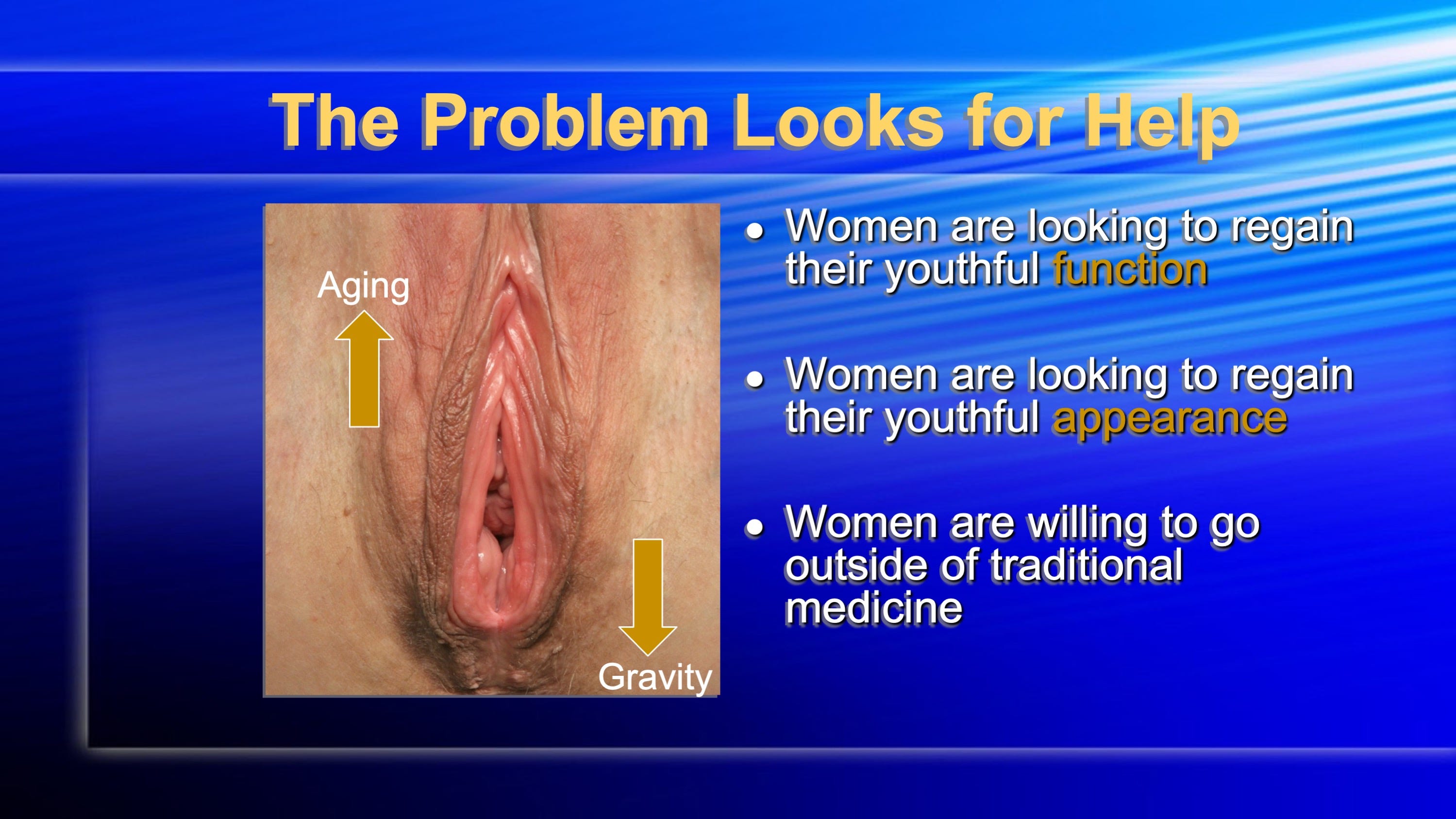
Women wanted not just to regain their youthful function but to regain their youthful appearance. Insurance never cared about those things. Traditionally trained OBGYNS poo poohed and looked down their noses at those who added these lasers and radiofrequency devices, platelet rich plasma, amniotic fluid, Bioidentical hormone therapy. Women worldwide were now willing to go outside of traditional medicine. The horse left the barn. Organizations such as ISCG and AIAVS flourished and taught the steady stream of doctors wanting to learn a different way. Those docs wanted control of their practices and their lives. They were tired of having insurance companies holding the keys. Cosmetic Gynecology cared not for boundaries between specialties. It was agnostic of specialties. Because of this way of thinking ACOG lost control. Gyns, Plastics, Cosmetics, Derms, Primary Care all banded together and planted on the fields abandoned by mainstream societies.
I will review the various procedures of Cosmetic Gynecology on the next post. Get some of the verbiage and definitions covered. A common library of terms is always useful now that this subspecialty is worldwide. Stay tuned. Subscribe.