


Health and Hormones Part 3
Get Your Moxie Back

Part 1 discussed what happens in menopause. Part 2 discussed what happens to your health risks. I did mention several times the positive effects of estrogen specifically for various conditions. Now let’s move to the final section and discuss your treatment options in general. You can take notes so you can discuss these options with your health care provider. Lots of choices as you see below:

The American College of OBGYN (ACOG) had these recommendations as a guide. Their website has a good summary of Frequently Asked Questions.
ACOG say this directly:
Estrogen-only therapy causes the lining of the uterus to thicken, which increases the risk of endometrial cancer. Adding progestin decreases this risk.
Combined hormone therapy is associated with a small increased risk of breast cancer. Women with a history of hormone-sensitive breast cancer should try nonhormonal therapies first to treat menopause symptoms.
Combined hormone therapy also may reduce the risk of colon cancer.Combined hormone therapy is associated with a small increased risk of heart attack for older women. This risk may be related to age, existing medical conditions, and when a woman starts taking hormone therapy.
Some research suggests that combined hormone therapy may protect against heart attacks in women who start combined therapy within 10 years of menopause and who are younger than 60 years. This benefit may be even greater for women taking estrogen alone.
More research is needed on this topic. At this time, combined hormone therapy should not be used solely to protect against heart disease.
Hormone therapy may increase the risk of other conditions:
Deep vein thrombosis (DVT)—Combined hormone therapy and estrogen-only therapy are associated with a small risk of stroke and blood clots from DVT. This risk increases with age and other factors, including heart disease, kidney disease, and obesity. Patches, sprays, and rings may pose less risk than pills taken by mouth.
Gallbladder disease—There is a small increased risk of gallbladder disease associated with estrogen therapy with or without progestin. The risk is greatest with pills.
Many of these risks are related to your health and family history. If you are thinking about hormone therapy, it is important to learn as much as you can. Discuss your options and the risks with your ob-gyn.
Systemic hormone therapy usually is not recommended if you have ever had:
Breast or endometrial cancer
Stroke
Heart attack
Blood clots
Liver disease
Hormone therapy also is not for pregnant women. Stop taking hormone therapy if you get pregnant or think you may be pregnant.
Bioidentical hormones come from plant sources. They are similar to hormones produced by the body. They include commercially available products that are approved by the U.S. Food and Drug Administration (FDA), such as oral progesterone, as well as compounded drugs. A compounded drug is made by a compounding pharmacist using a health care professional’s prescription.
Compounded drugs are not regulated by the FDA. Customized compounded hormones pose more risk because they vary in strength and purity. That means you can take too little or too much of a hormone without knowing it. There also are safety concerns about a kind of compounded drug known as pellet therapy.
There is no scientific evidence that compounded hormones are safer or more effective than standard hormone therapy. The American College of Obstetricians and Gynecologists (ACOG) recommends FDA-approved hormone therapy over compounded hormone therapy.
So above is the official Party Line. Controversial and not everyone agrees. If you did not read my Part 2 post on this topic should go back and read the research I quoted that goes contrary to some of ACOG’s position. An example is the multitude of research showing natural estradiol to reduce the risk of breast cancer, stroke, and heart attacks and synthetic hormones such as Provera being the problem. Dr. Jeffrey Dach lists them on his website here. So personally, I am a proponent of estrogen supplementation, specifically Estradiol (E2) in the perimenopause and menopause if the woman has no history of breast cancer, uterine cancer, heart attacks, strokes, blood clots, gallbladder disease. It improves quality of life and duration of life. It can actually reduce your cardiovascular risks, thinning bones and fractures, colon cancer risks, cataract and macular degeneration risks. Of course it works very very well for hot flashes, sweats, chills, vaginal dryness, painful sex. It is known to improve that sense of well being, reduce the sense of impending doom, remove that dark cloud that seems to follow. I avoid synthetic estrogens and Premarin. Those are NOT what the body used to make on its own. The woman’s ovaries used to make Estradiol (E2) and Estriol (E3). Most compounded formulations have both E2 and E3. There is belief in many hormone specialists that E3 has more breast cancer protective effects but this is the minor estrogen produced and used by a woman.
So when someone says they want something “natural” what does that mean? Natural Estrogens are found in humans and animals. In humans it is Estradiol mostly and also Estriol. These is not found in plants. However, plants such as Soy and Yams can provide the basis for highly altered chemicals that then are “Bioidentical” or look the same in structure as those found in humans. Bioidentical means the chemical structure is the same, indistinguishable of whether is came from a human or a plant source. They look the same and function the same though the source was different. The components of Bio HRT are Estrogen, Progesterone, Testosterone, DHEA, and in some instances thyroid hormones, Human Growth Hormone, and Cortisol. I will cover Testosterone alot more later.


Here is something to consider though it is controversial. The Europeans use alot of creams for hormones. Why? To bypass the liver. American have followed suit. Not everyone is convinced that creams, patches, troches, and pellets used to bypass the liver is better. Up to one third of women absorb creams and patches poorly. Many prominent specialist love their pills to get consistent blood levels.
ACOG does not believe in creams and pellets and anything compounded. ACOG does not like the use of compounded Bioidenticals because of concern that it is not regulated and that there is no proof it is better than what the drug companies sell. They do not have an open mind on this and rarely is there a talk or presentation on this at the national meetings. Other societies like the Menopausal Society are a bit more accepting but from arms length. There is always politics involved. Ask yourself who benefits from the positions taken. Drug companies?
Let’s talk about alternative therapies to consider for Hot Flashes, the most common symptom of menopause. Let’s say the patient has had breast cancer or a stroke. The list below is a pretty good compilation of options. I personally use natural Progesterone pills because of the safety. Not only does it reduce the hot flash and night sweats it also has protective effects on the breast and prevents uncontrolled cell division. It also protects the uterus from hyperplasia and cancer. In someone with a uterus, it almost always given with Estradiol as part of BioHRT therapy. The real cool added plus is that it can help calm the mind, get you to sleep, and keep you asleep. Don’t ever take Progesterone in the day or you may be groggy all day and feel like a slug. Progesterone does not increase your risk of stroke or heart attack or cancer in general. If you have positive Progesterone receptors in your breast cancer then you should not take it. Provera has the same positive effects as Progesterone but has the problem of being synthetic and the increased risks of breast cancer, heart attack, and stroke. By the way, the brand name of Progesterone is called Prometrium.

So as you can see there are options from blood pressure meds like Clonidine, Catapress, Aldomet to over-the-counter supplements such as Rice Bran Oil, Black Cohosh, Soy products. The effectiveness varies and the proof it works are all over the map in terms of research. For example, Soy products do not do great in reducing hot flashes but probably is beneficial in lowering cardiovascular risks. Soy is in the Phytoestrogen family. There are lots of Photoestrogens OTC to choose from.

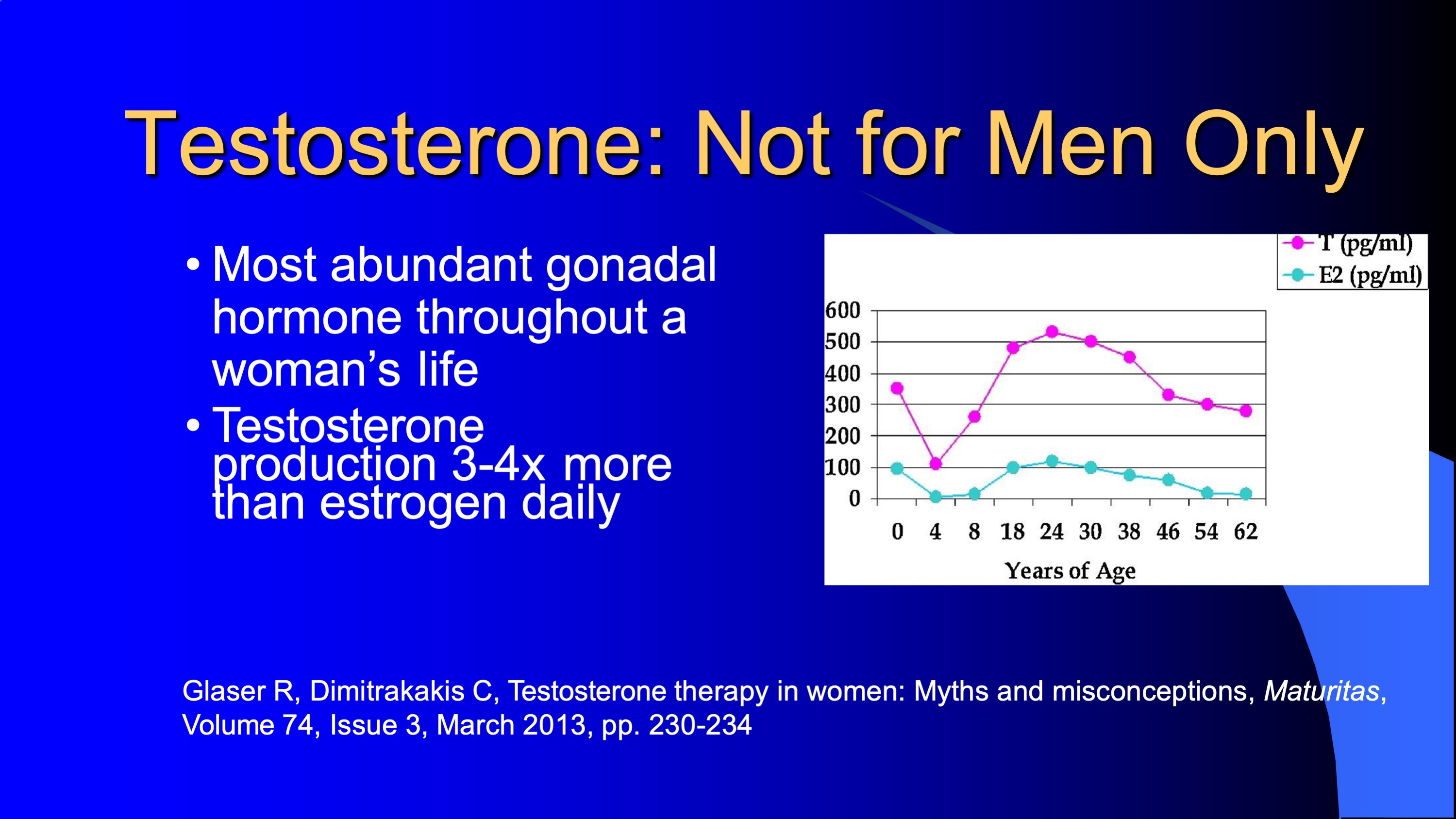
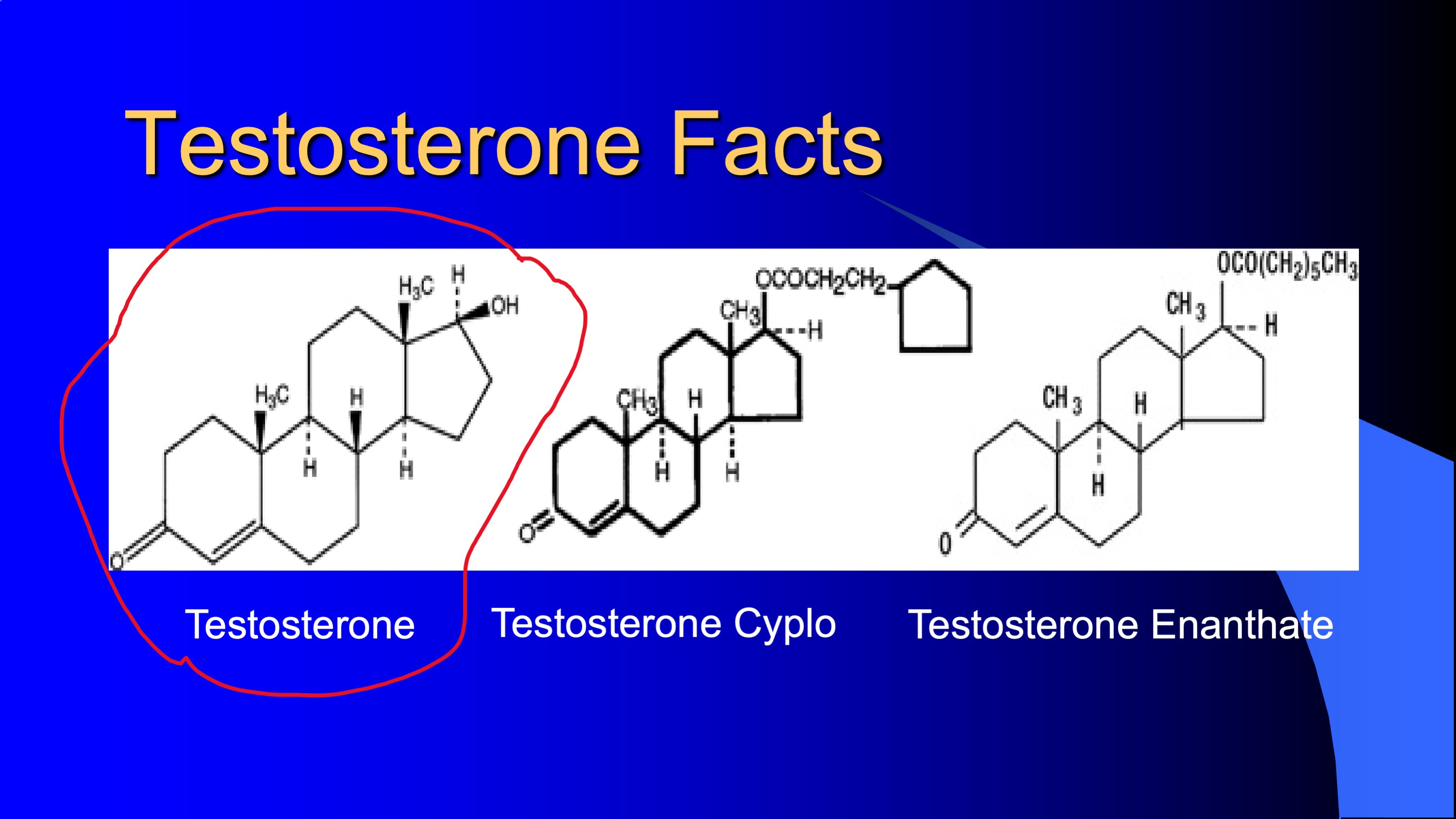
Finally, let’s cover the use of Testosterone. Here is some history:

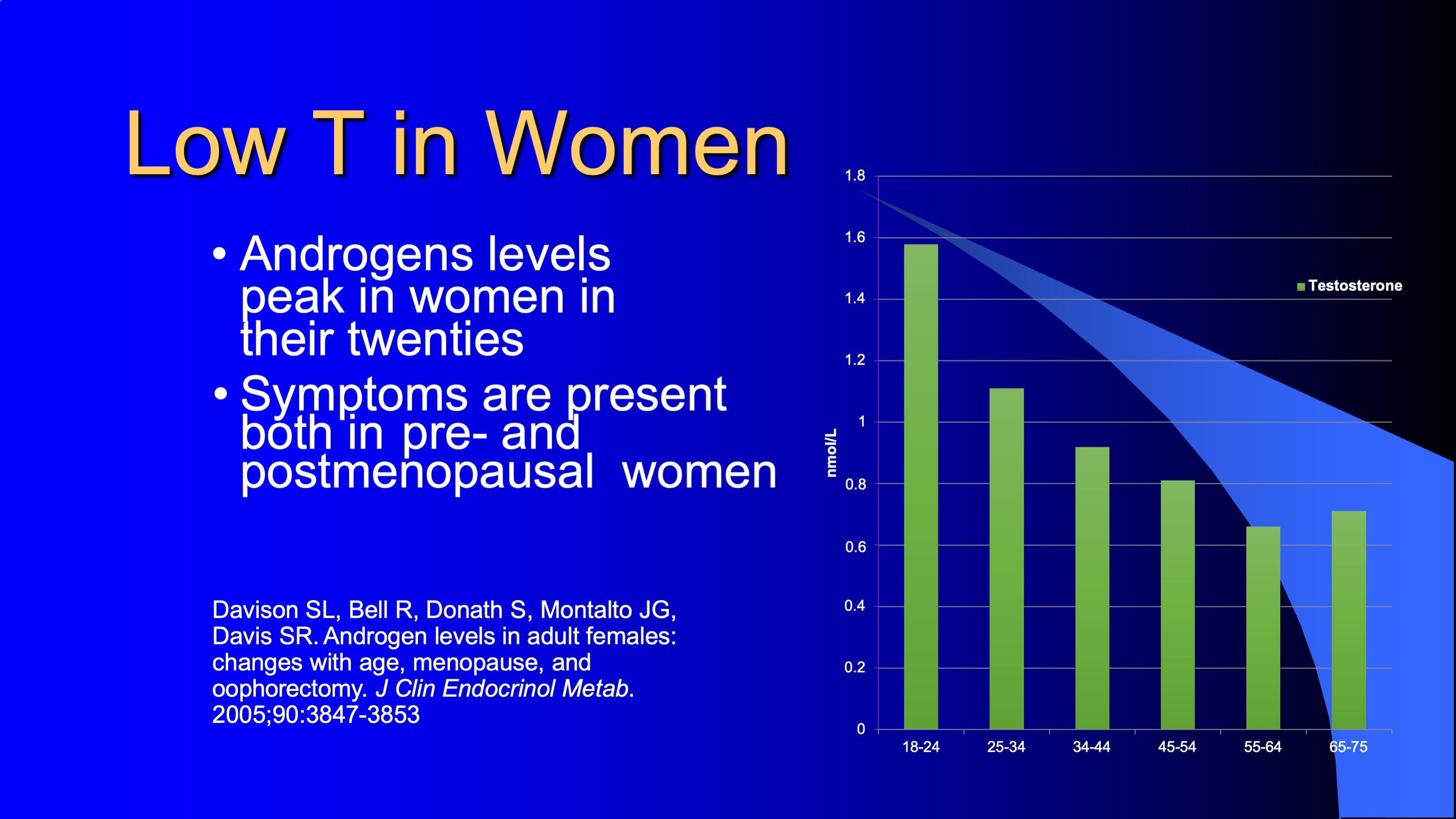
So we age and we loose testosterone. Men and women both. Testosterone is not just a man thing. Women make lots of it actually.

Low T does not discriminate. It affects women too. Low T in women results in low libido, loss of the lean body, weakening of bones, loss of muscle strength.
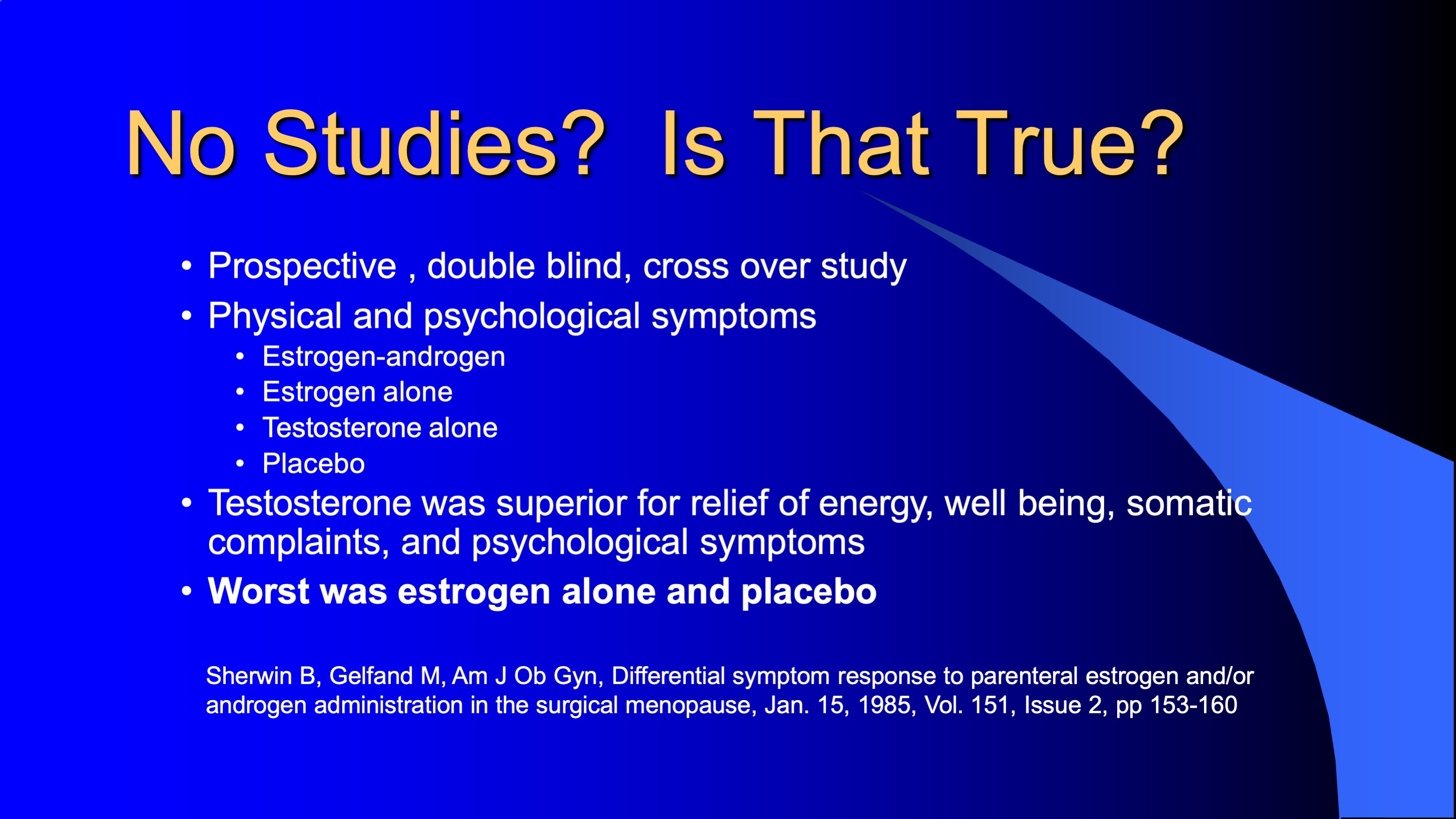
Do you really need Testosterone to feel good as a woman? Look at the study below that specifically looked at physical and psychological symptoms. Testosterone alone beat Estrogen alone and Estrogen-Testosterone together! This was a real good study. Women got their Moxie back!
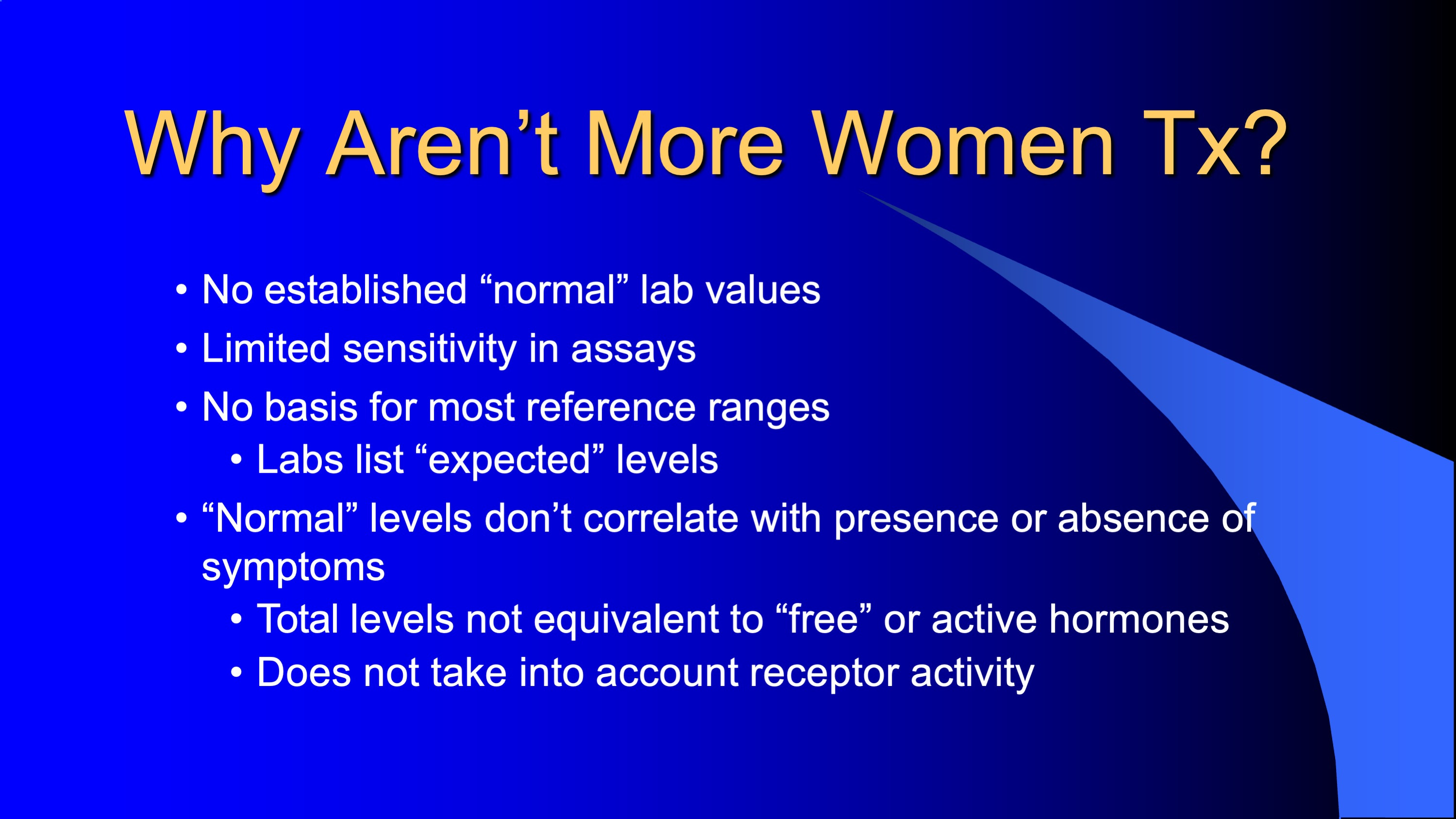
Not too many women are on Testosterone supplementation. Here are some reasons:
Here are some myths about Testosterone use in women:
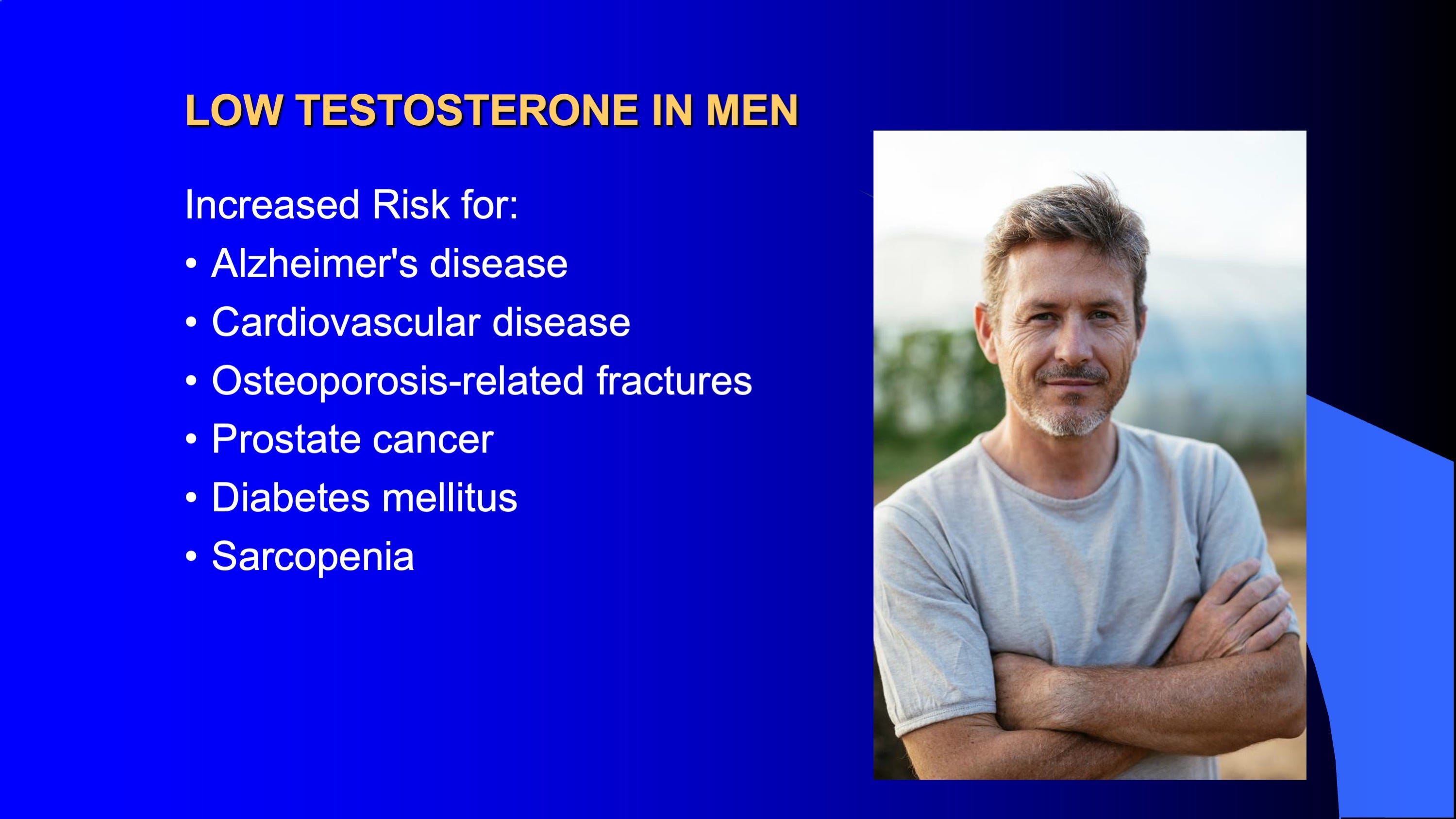
Take a look of what happens to men who have Low T:
Take a look of what happens to women who have Low T:

Are you surprised? Here are the positive effects of Testosterone supplementation for women who are managed closely by an expert:

Now remember that these effects are seen with “Natural” Testosterone and not a synthetic Testosterone. Those are different things!
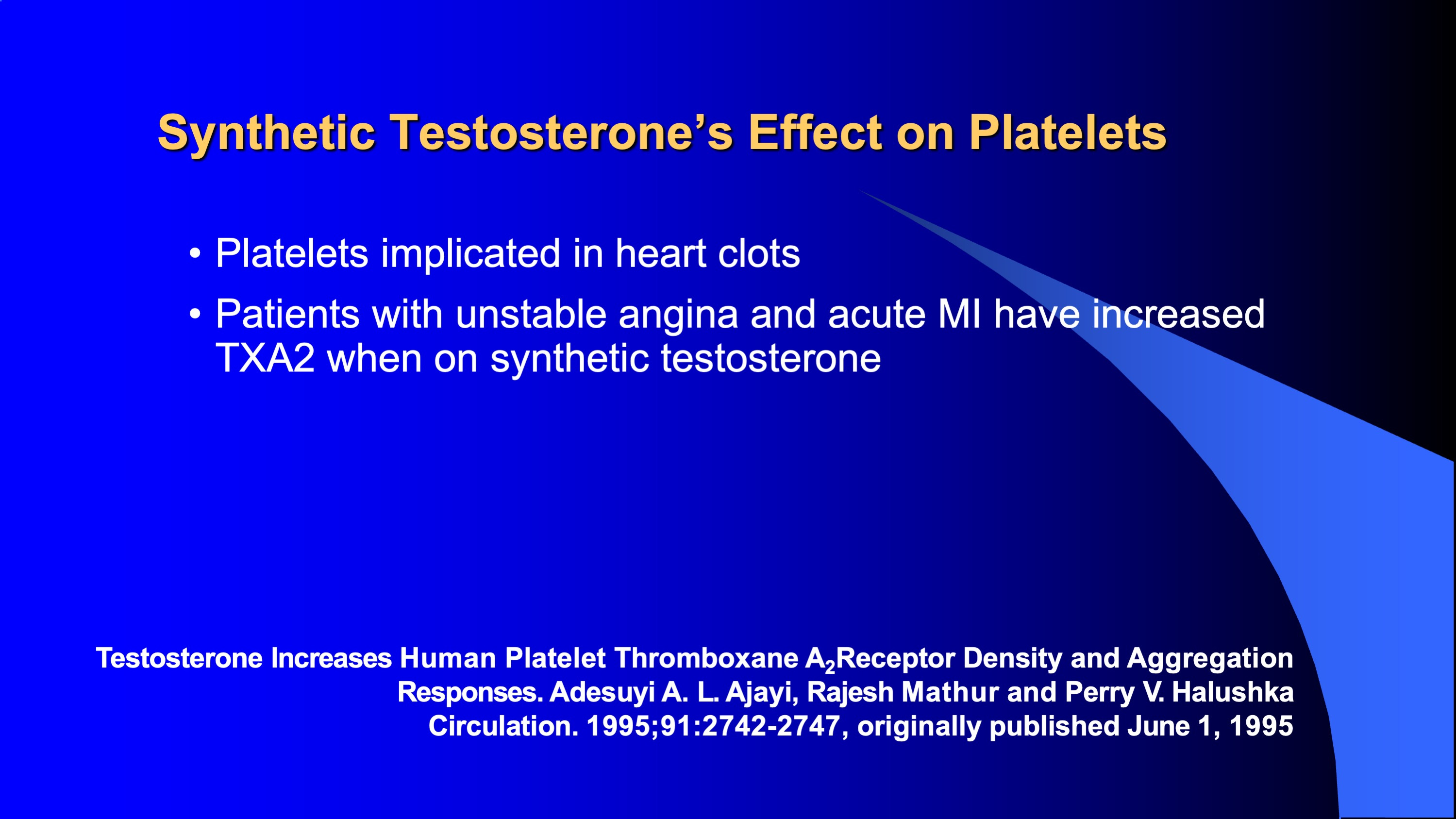
Synthetic Testosterone, the injected stuff, has lots of problems. Here is a list. Allergies can happen. Notice that you get roller coaster effect because of the variable levels from injections. You get broken red blood cells.
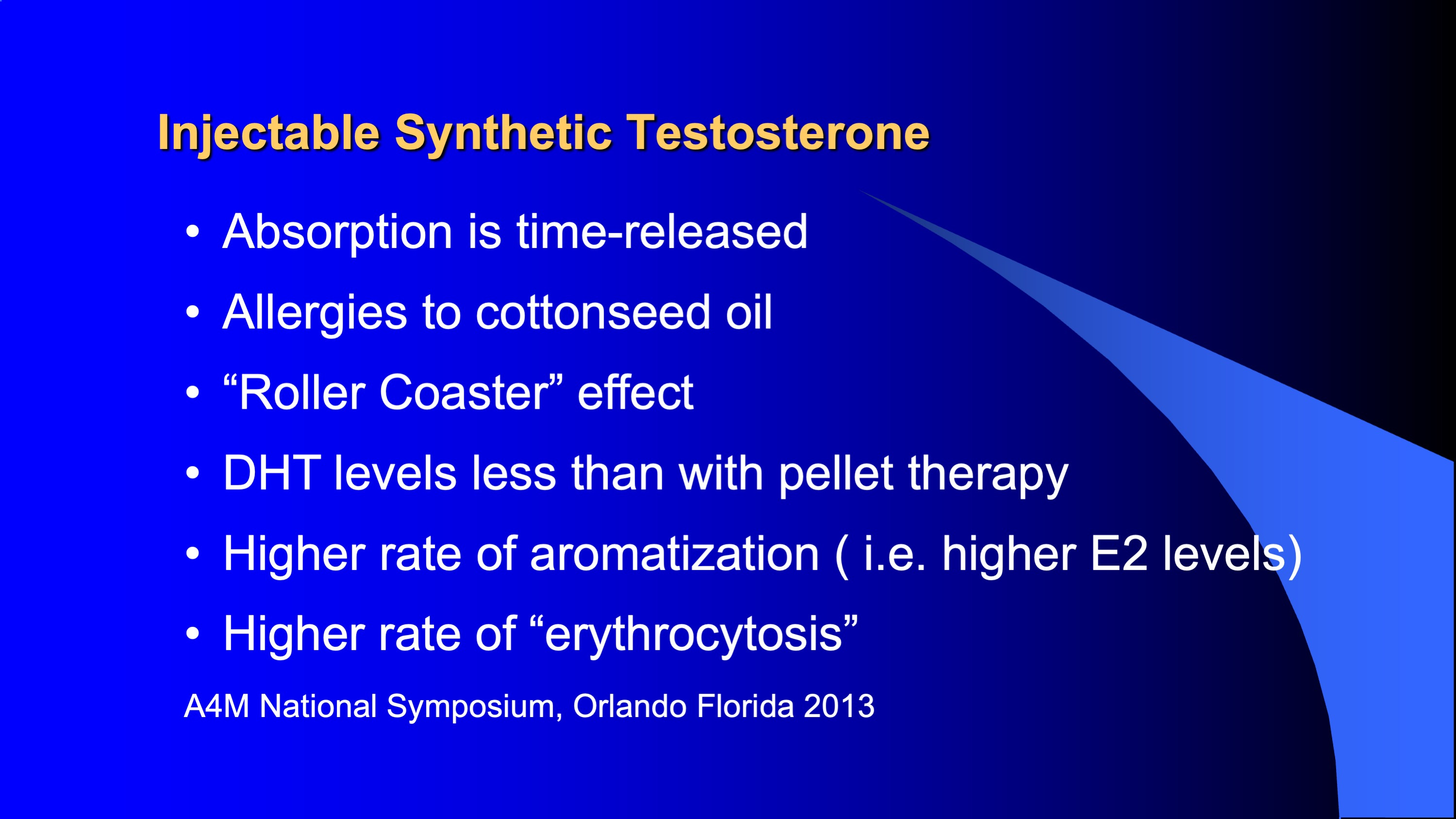
Those effects of Synthetic Testosterone cause an increase risk of clots and heart attacks. Don’t take them those injectables! Creams and Pellets do not have this problem because they are made from Bioidentical Testosterone and not a synthetic.
I use lots of Testosterone creams and most absorb it well. But some do not. So consider Pellet therapy for Testosterone.
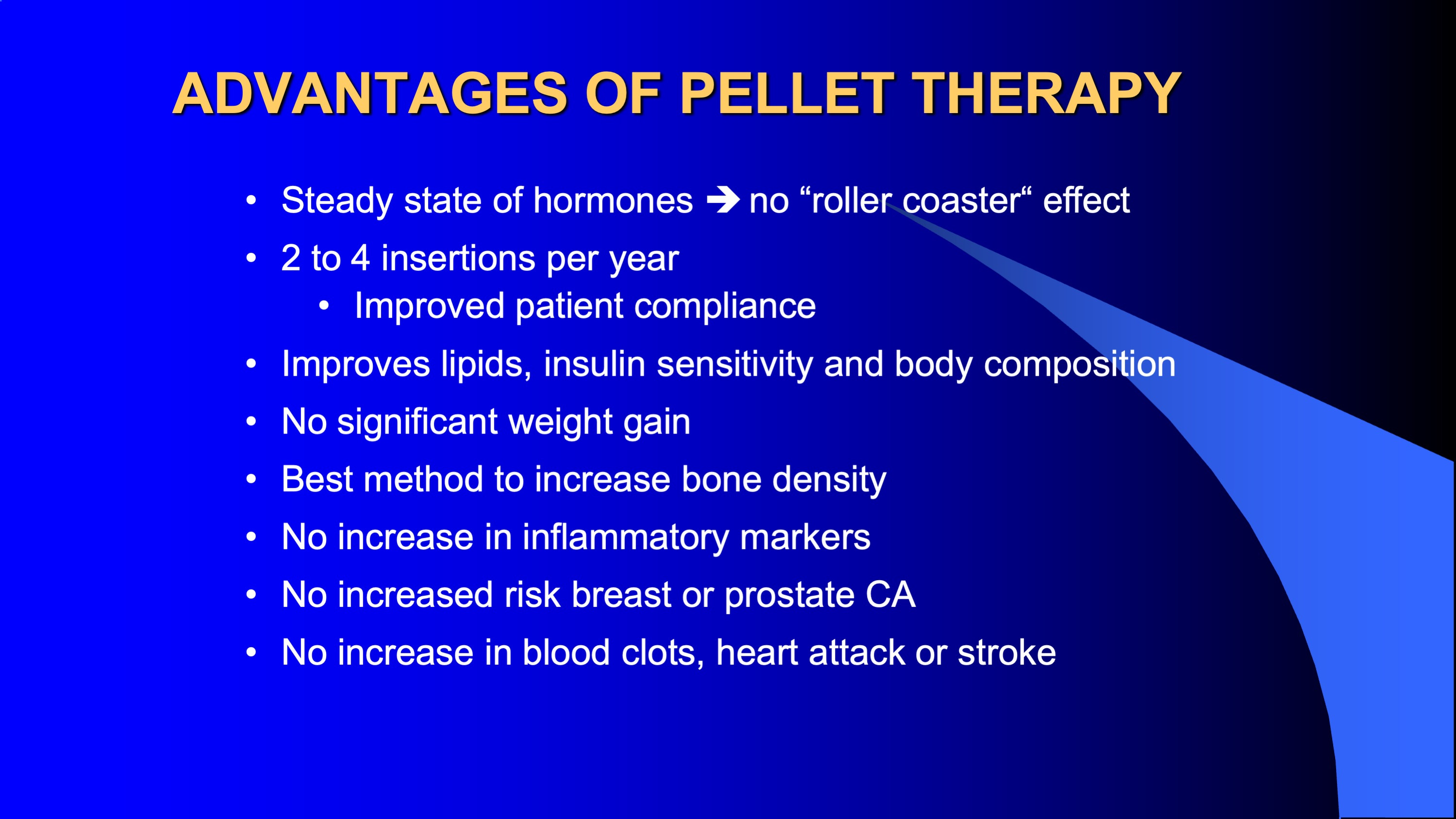
Here is a summary slide of the various ways to get Testosterone and the Pros and Cons. Delivery methods do matter.

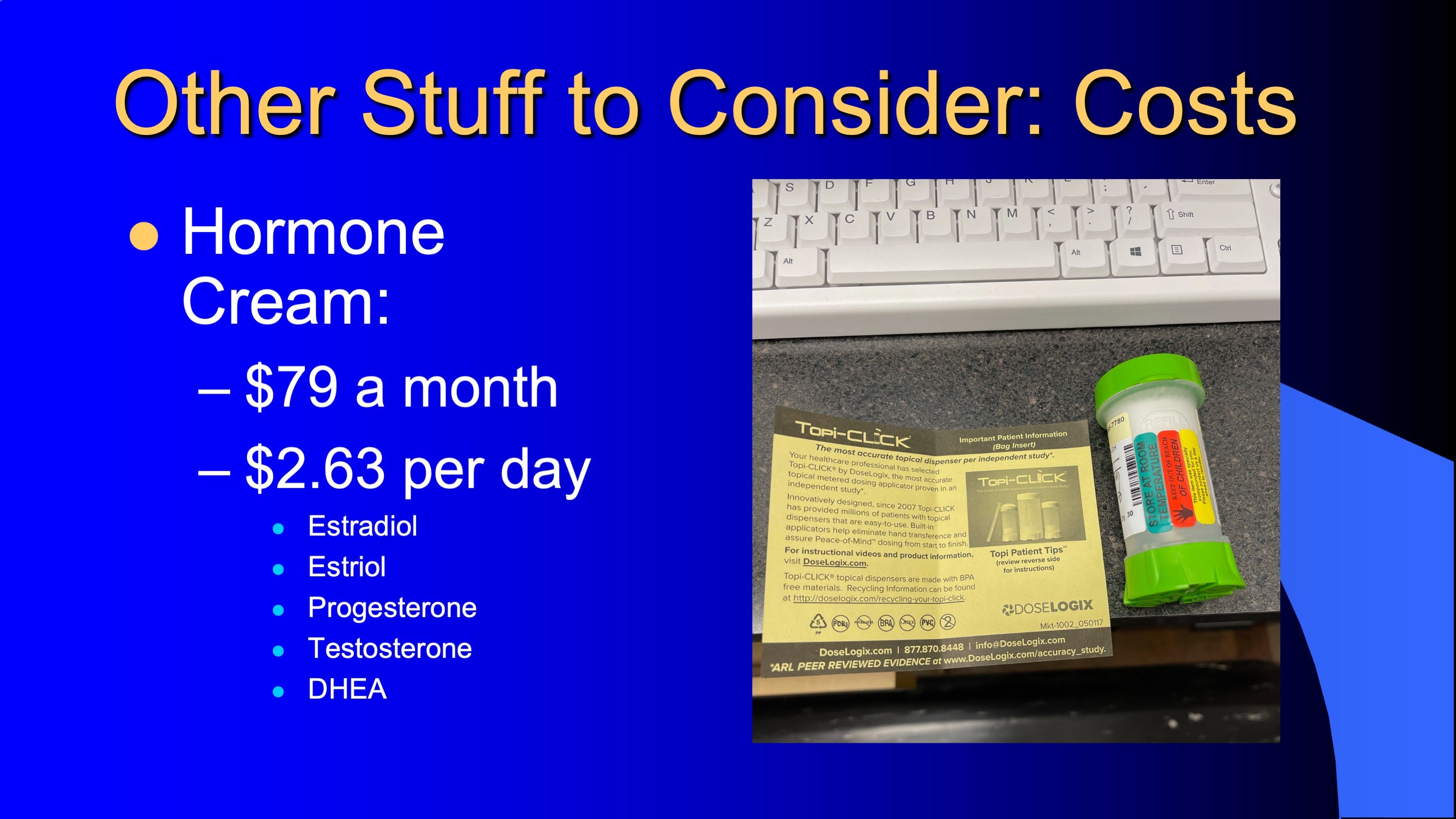
Here are the financials to consider. Creams are cheaper per day. But less convenient. You have to rub the creams on every night below your belly button, or inner thighs, or inner arms. Creams can be managed by phone calls. Pellets needs you to come into the office every 3-4 months. Lots to consider. None of this Bioidentical stuff is covered by insurance.

So let’s close and summarize things:
Again, let’s give kudos to Dr. Jeffrey Dach who freely gives out this information on his website. Get his book.
Give us a follow in IG. Check out my website at www.urogyn.org. For doctors who want training go to www.alinsodinstitute.com. Become a paid member for more of this really good stuff!


If you want to watch this Part 1, 2, 3 as a video webinar go to Health & Hormones Webinar on my main website by clicking on the link.
On Monday, April 25, 2022, I will introduce you to Carboxytherapy and its applications for Feminine Wellness. Free access ends this weekend and Full Access will require a paid subscription so I hope you upgrade. It is worth it.